
It's safe to drop our masks but not our guard (I will never trust the CDC again)
Two years ago the CDC's rationale for mask mandates was beyond reproach. A closer look at their methodology tells the story of their deceptive practices.


Just a few months ago I saw a person standing alone in a parking lot, masked and holding a lit cigarette. It’s pretty clear that people have reached their own conclusions about masks and many cannot be swayed from their initial feelings even though mandates have largely been dropped. My intention in writing this piece is not to settle the debate around masks and mask mandates. That’s an impossible task.
However the topic does give us insight into how our agencies of public health will resort to devious methods to push their agenda on a well-intentioned public that does not have the capacity to challenge their edicts. Just two years ago our Centers of Disease Control and Prevention published a Morbidity and Mortality Weekly Report, “Association of State-Issued Mask Mandates and Allowing On-Premises Restaurant Dining with County-Level COVID-19 Case and Death Growth Rates — United States, March 1–December 31, 2020” that seemingly put the issue to rest. It didn’t. In fact it stands as unassailable proof that the CDC will serve as a propaganda machine disguised as an agency of public health…
Most of my physician colleagues will remember the first time they walked into an operating room. That’s when the circulating nurse looked us up and down and made it very clear that we were to do as we were told.
“There are two basic rules. 1) Do NOT touch anything unless someone asks you to touch it. 2) If you have to sneeze or cough, do NOT look away from the patient.”
I had no problem with the first rule. I didn’t want to touch any of the trays of shiny medieval tools they called “instruments”, but it was hard to suppress my natural tendency to turn away from the most important person in the room, the patient, when I had to sneeze.
The need for the second rule was simple. Whatever comes out of your lungs eventually gets blown out the side of your mask. It’s unavoidable. The best we can do is direct the plume of yuckiness away from the surgical site. That meant looking directly at the open wound and letting it rip.
This is why I was baffled by how many doctors simply accepted the idea that flimsy surgical masks placed on asymptomatic people would have any effect on the spread of Covid-19 in public.
But we were in a crazy time in the spring of 2020 and everyone felt like they had to do their part in curbing the spread of this respiratory borne illness. When I started seeing people wear masks outside I knew that we weren’t going back to normalcy anytime soon.
I’m an anesthesiologist. That means I have had to wear a mask for forty hours a week for the last two decades. I don’t do it because everyone thinks it’s a good idea. There is a consensus around what masks can and cannot do. In the OR they serve as a mechanical barrier between us and the patient. It keeps spittle from an open wound and protects our faces from blood and bodily fluids.
Masks on anesthesia providers have been shown to have no role in preventing surgical site infections, even though we typically are sitting just a few feet away from the surgical field. Several western countries do not require anesthetists to wear masks in the OR. This is based on long-standing research.
However wound infections are different from respiratory borne illnesses. In the OR, when we are caring for a patient with an active pulmonary infection, we take our masks off, don custom fit N-95 respirators and crank up the negative pressure in the room to mitigate the risk of contracting whatever the patient has. That helps.
To be fair, we cannot say that masks confer zero protection to those around us. It’s entirely possible that they may help in some infinitesimal way. That logic was enough for most people. If it saves a single case of Covid-19, isn’t it worth the minor inconvenience?
But what might be a minor inconvenience for most isn’t for some people who have limited pulmonary reserve. Ask any mother of a child with asthma. You can show her a hundred studies that demonstrate that masks do not impede respiration, but when her child is having an acute attack you can be sure the first thing she will do will be to rip the mask off their face. She’s not being unscientific; she’s being intuitive.
Despite nearly three years of heated debate we have been unable to come to any consensus about the effectiveness of mask wearing in preventing Covid transmission. On the other hand, we do know that it has measurable, detrimental effects on different aspects of our health, especially with prolonged use:
By now we should be able to agree that masks may have some protective benefit but mask mandates do not. This was recently established by a Cochrane meta analysis of large observational studies including hundreds of thousands of people. The authors summarized:
“Ten studies took place in the community, and two studies in healthcare workers. Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu‐like illness/COVID‐like illness (9 studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (6 studies; 13,919 people).”
We may be able to excuse the public for doing what seemed sensible at the time even though throughout 2020 and early 2021 Covid-19 infection rates in states where mask mandates were implemented mirrored those in states without mandates.
Then in March of 2021, the CDC published this astonishing Morbidity and Mortality Weekly Report wherein CDC authors claimed there was an association between a decrease in Daily Growth Rates of Covid-19 deaths and cases and mask mandates.
Exposing the CDC’s tricks
I will devote the remainder of this article to explaining the disingenuous and devious methods our Centers for Disease Control and Prevention employed to convince the public that mask mandates were somehow protective.
This was an eye opening moment for me because it demonstrated, beyond any shadow of doubt, that this organization will act as a propaganda machine while posing as an agency for public health.
In order to see the deception a certain level of mathematical fluency is necessary. I will try to spell things out as simply as possible.
The CDC used county wide Covid-19 case counts over a period of 10 months between March and December 2020. They then claimed that a 1.5% drop in the rate of growth in cases (and deaths) were associated with the institution of mask mandates in those counties. They expressed their findings graphically here:
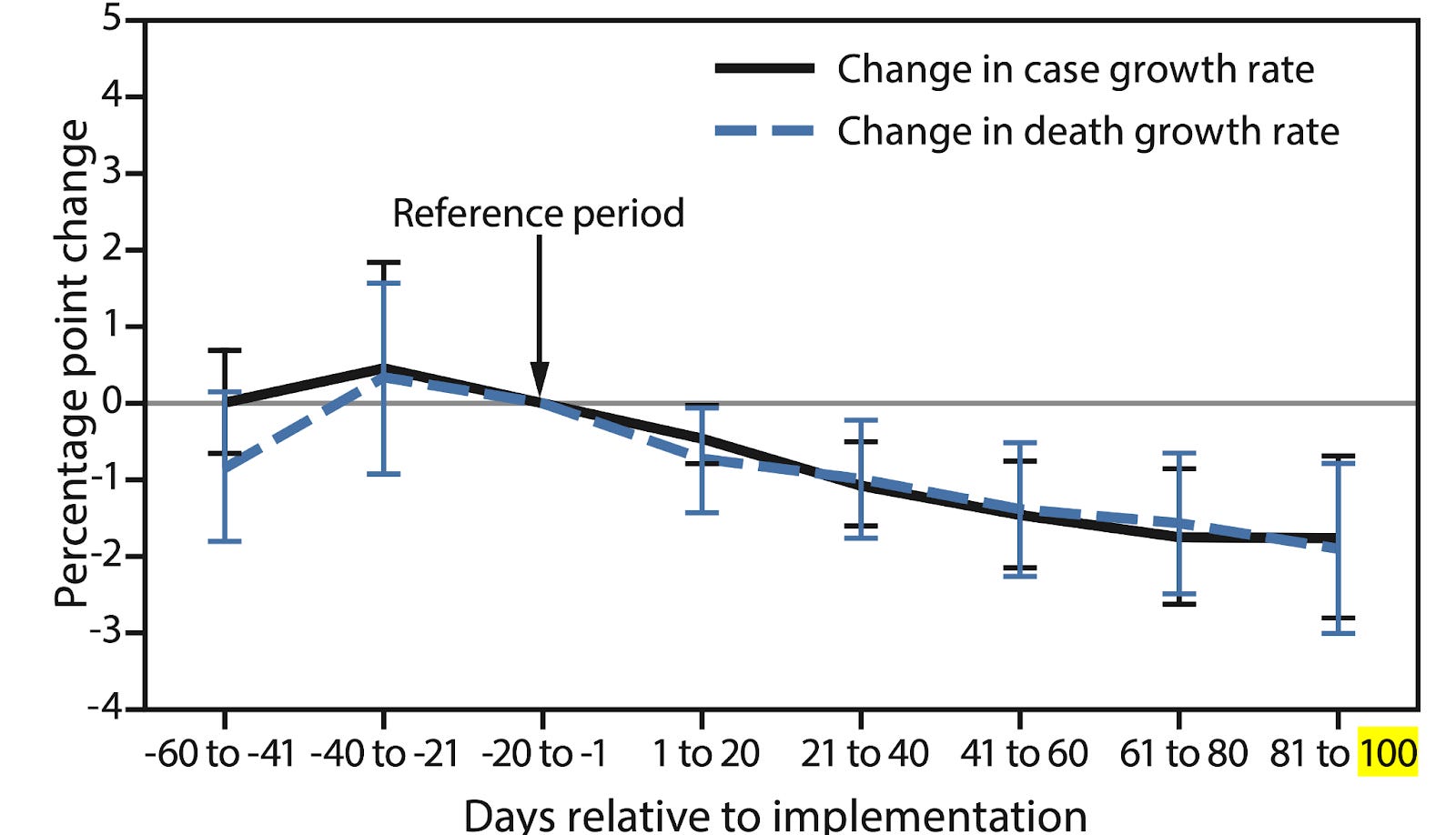
This simple plot is the result of some straightforward number crunching on a very large data set. There are two lines, one in solid black, the other in a dotted blue. For the purposes of this piece, I will be addressing the black line, which represents the “Change in case growth rate”.
The “Reference period” is the growth rate of Covid cases at the time when a mask mandate was implemented upon a county. Mask mandates were, of course, imposed at different times in different parts of the country. That is why the x-axis, time, is not given as a calendar date but as days elapsed since or days prior to the institution of the mandate.
The black line is the composite of all counties that imposed mask mandates during the 10 month period of observation. The plot is weighted by population. This means that counties with greater populations will have a greater effect on the plot.
At first glance it seems that in general, after mandates were imposed, the case growth rate fell. This is indeed how this story was rapidly echoed on most major mainstream media platforms within a few days of this publication.
To be crystal clear, the CDC wasn’t saying that number of new Covid cases fell after the Reference period—they were telling us that they weren’t increasing as quickly. If you think this is a rather low standard for a preventive measure to meet, I would agree. While we are on low standards, let’s take a closer look at the methodology the CDC employed to do their “research”.
First, the growth rate of cases prior to the mandate implementation is unclear. Error bars which demonstrate the range of statistical significance span both sides of the x-axis prior to the reference period. This means that nobody, including the CDC study authors, could tell if the case growth rate was already in decline prior to the mandates. In other words, the authors could have just as easily concluded that mask mandates were associated with a fall case Growth Rate 40 days before the mandate was imposed. Of course if that were the case the drop in case Growth Rate would have absolutely nothing to do with mask mandates.
But the authors never state that mandates caused the fall in case growth rate. They only point out that they were associated with it. However, we can all agree that that is not how it was explained to the public.
Now I will get more technical…
The CDC chose to define their metric of interest, Daily Growth Rate in cases (DGR), as a function of the cumulative cases (CC(t)):

“ln” is the natural logarithm. This is a peculiar way of defining what should be a straightforward variable. Moreover, it leads to the unavoidable certainty that if the number of cases is not growing exponentially, DGR will necessarily decrease.
Defining DGR this way is particularly useful if one is trying to prove that mask mandates (or anything else for that matter) are associated with a fall in Daily Growth Rate, no matter how miniscule.
For example, during the observational period in the CDC study, the peak of new Covid cases on a given day in the U.S. was about 200,000. If we had two hundred thousand new cases every day from the first day of the period we would have about four million cases in three weeks. Plotting CC(t) against time:
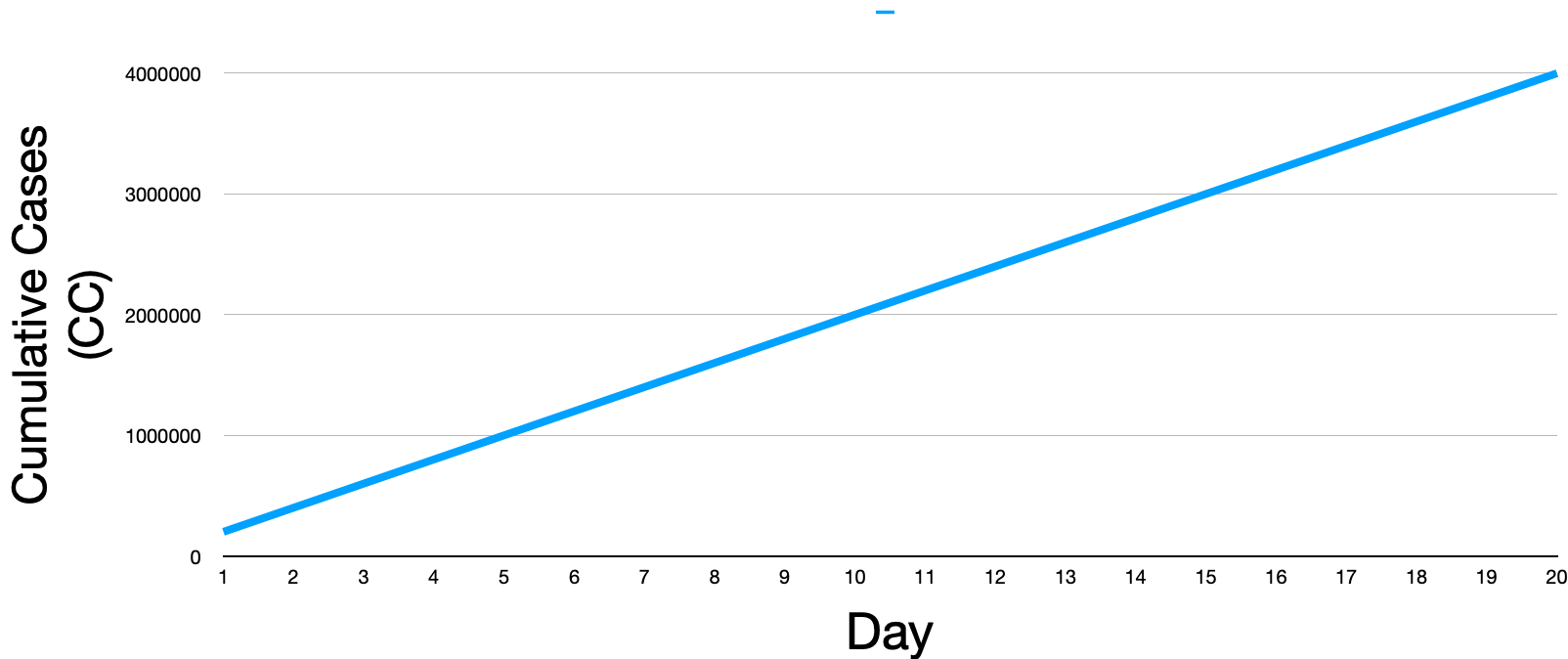
Thankfully, we did not have nearly that many new cases on most days during the pandemic, but if we apply the CDC’s definition of Daily Growth Rate (DGR) to this disastrous rate of case growth we get this:

As you can see, DGR keeps dropping. This is because even if we were adding 200 thousand new cases every day, this represents linear growth, a snails pace compared to exponential growth. Exponential growth is required to have a DGR (as the CDC chose to define it) that doesn’t fall. This is what exponential growth would look like:

The problem should be apparent. Nothing in nature can grow exponentially for very long. Nevertheless, this kind of case growth would be required for mask mandates to not be associated with a fall in DGR.
With regard to cumulative number of infections, we may see a brief period of exponential growth in cases when a new pathogen attacks a naive (not immune) population initially. Eventually, the population gets exposed and many develop natural immunity and cannot be part of the naive pool. Others will die and also be taken from the pool of uninfected people. DGR will eventually (and as I demonstrate below, quickly) diminish independent of any action by health agencies.
When we plot the actual number of cases in this country over time for the first year of the pandemic (3/2020 to 3/2021) we get this:

Applying the CDC’s formula for Daily Growth Rate, we get this:

As we would have predicted, the slope of the line is negative for the entire year except for a small window of time at the beginning of the summer and the middle of the fall. This means that for nearly all days during this time period DGR was falling. This plot for the whole country matched, more or less, what happened in most states and counties.
This brings us to the next CDC ploy: cherry picking the time window of observation.
Different counties imposed mandates at different times as mentioned earlier. However the majority of counties instituted them during the spring and summer of 2020. This would have posed a problem for the CDC authors because there were two bumps in DGR, one in the early summer and another in the autumn.
In other words, choosing a shorter time of observation, say thirty days, would have led to an increase in DGR for states with earlier or later dates of mandate imposition. Choosing a 150 day window would have led to equivocal results for states that implemented the mandate at the beginning of the summer because of the fall bump.
They got around this by choosing a 100 day window of observation. There is no precedent for this kind of study. Why did they choose 100 days?
The CDC authors undoubtedly examined data for the whole 10 month period first and then chose a window of analysis that neatly fit between the two bumps, at least for the majority of counties.
Yes, I am speculating, but it would be absurd to think that the CDC authors simply chose a 100 day window a priori and then publish their findings, especially when they had no constraints to begin with. That’s how they got their composite plot to trend downwards.
Any scientist would regard this kind of analysis as specious if not deliberately misleading. Unlike other published scientific papers, the CDC MMWRs are not subject to a peer-review process, yet their “findings” are disseminated by mainstream media as irreproachable scientific gospel.
The CDC authors needed one more trick to pull this off. We already knew that infection rates in states without mandates were about the same as in states with mandates. The CDC had been publishing this data on their own website. If they applied their formula for DGR to states without mandates it would have revealed their deception. This is why they chose not to examine Daily Growth Rate in cases in any county that did not have a mandate. In other words, there was no control group.
I co-authored a paper on this data with Josh Mitteldorf, PhD (check out his substack, Unauthorized Science). We examined CDC data from seven of the most populous states that never had a mask mandate. We arbitrarily picked a Reference time as the first week in August and got this:

I wonder why the CDC chose not to apply their methodology to these states to prove that they weren’t just handwaving. Could it be because it would show identical findings to the masked states?
Had they offered this data they would have had to admit that the rapid fall in DGR could have also been due to the vernal equinox in March, fireworks in July or eating more turkey around Thanksgiving.
BUT WHY??
We finally arrive at the biggest question, what was the motivation behind publishing this kind of “science”? What was to be gained by misleading the public into wearing masks? Surely they knew that some of us would be able to smell BS whether we were wearing masks or not. Why risk the reputation of the CDC over mask mandates? Was the CDC beholden to companies that make surgical masks too?
The MMWR was released on a Friday. On the following Monday, March 8, 2021, the CDC tells us, as NBC News reported:
“‘As more Americans are vaccinated, a growing body of evidence now tells us that there are some activities fully vaccinated people can do,’ the CDC’s director, Dr. Rochelle Walensky said during a White House Covid-19 briefing Monday.
“‘The latest science [emphasis added],’ Walensky said, ‘suggests that fully vaccinated people can congregate indoors with other fully vaccinated people without wearing face coverings or practicing physical distancing.’”
And there you have it.
Three days after the flawed MMWR was released, congregating with other human beings indoors with an uncovered face became a privilege reserved exclusively for the fully vaccinated.
The “latest science” must show that masks offer some protection, however miniscule. Target gift cards, Krispy Kreme doughnuts and free ice cream weren’t working. Enough of the carrots. They needed some sticks. The CDC had to demonstrate that there was a benefit to mask mandates so that our authorities could selectively apply them to those who didn’t comply with their vaccine agenda.
Number 5,384 from "How to Lie with Statistics, Virus Edition." Were Huff alive today he could write multi-volumes on Everything Virus. This is a terrific example. And you give a classic, too, in the annals of "what nearly everything thinks is true is wrong" (turning to the side to sneeze, which I suspect is also true when just using ones arm or hand to block the snot splatter). Thank you for this.
BREAKING NEWS - TWO HOUR: EMERGENCY DEFENCE AGAINST WHO - TWO SWISS: NAJADI & STUECKELBERGER, TWO AMERICANS: LEE VLIET AND ANN VANDERSTEEL
New Breaking Revelations: From Pascal Najadi: in the name of Humanity
https://rumble.com/v29k26a-k-o-n-k-r-e-t-emergency-defence-against-who-no-more-virus-psyops-the-facts.html
This is the two hour recording of our discussion initiated by Pascal Najadi, retired Swiss investment banker who filed criminal complaint against the President of Switzerland, regarding the WHO declaration of the Marburg pandemic. Guests with Pascl Najadi are Dr. Elizabeth Lee Vliet MD - physician from the USA, Dr. Astrid Struckleberger, MD former WHO physician from Geneva, Switzerland, and Ann Vandersteel, Co-Chair, The Zelenko Foundation, USA. We think you will find it very informative to watch.
From Pascal Najadi: “We will completely dissect the subversive terrorist WHO mass murder Organization that failed to do a Coup d‘Etat on our democracies. All bad evil actors of the UN, WHO, WEF, Pfizer, Pharma etc and respective Government members that conspired with them against the divine Humanity, us, will be meeting the wrath of Justice and will forget how their names are spelled, I promise this to all of you, for the Lord our creator will guide and protect us. We Humans are one, Divine. Please spread this to all corners of this world, fellow Humans like us need to know the Truth. Truth. Godspeed, Sincerely, Pascal”