


Placebos? We don't need no Placebos! Unless...
An exploration into the mind of a vaccine enthusiast


A very interesting study was posted in preprint last month which compared a large group of vaccinated individuals in Florida. The authors, Retsef Levi, Florida Surgeon General, Joe Ladapo, MD et al found that over a twelve month period following vaccination Pfizer recipients suffered a significant increase in all cause mortality compared to those who got the Moderna shot:

The blue line in each plot are the cumulative risks of those receiving the Pfizer formulation, the red is the Moderna. At first glance, the results are stunning. Pfizer recipients not only had a greater risk of dying from Covid-19 but also from cardiovascular etiologies and all other non-Covid reasons when grouped together. It follows that death from any cause (All-cause Deaths shown in the upper left) was also greater for Pfizer recipients.
James Lyons-Weiler wrote an excellent piece which contextualized the results and described the strengths of the study and possible implications:

Summarizing Lyons-Weiler:
Pfizer recipients had a 37% greater risk of dying in the twelve months following vaccination. The risk was statistically significant and resulted in 229 more deaths per 100 thousand people.
This wasn’t a marginal or abstract difference. 735,050 pairs of adults were matched by age, sex, race, ethnicity, socioeconomic status, vaccination month, vaccination site and previous exposure to Covid-19.
There was a statistically significant increased risk of all categories of deaths examined: cardiovascular, Covid-19 related and non Covid-19 related.
The increased risk in mortality began to appear within a few weeks and expanded over time. This means that this was not due to differences in reactogenicity but from a longer term physiological impact.
The protective benefits, as demonstrated by Covid-19 mortality, diverged with time since vaccination. Moderna recipients were better protected from death from emerging variants like Delta.
While the authors concede that differences in comorbidities between the groups could not be accounted for, negative control outcomes (suicide and homicide) were not statistically significant. This suggests that the Pfizer and Moderna groups were equally vulnerable to non-biological sources of mortality, meaning that the observed differences in all-cause, cardiovascular, and COVID-19 mortality are not likely explained by confounding from social or behavioral variables.
The study also used Rosenbaum’s sensitivity analysis framework. This demonstrated that “an unmeasured binary confounder would have to be 1.5 times more likely among Pfizer recipients and 6.4 times more predictive of death than all observed variables to eliminate statistical significance”.
According to Lyons-Weiler:
“That’s an implausibly powerful, hidden variable. It would need to behave like a combination of stage 4 cancer, chronic renal failure, and heavy opioid dependence, and still correlate with vaccine product selection in a matched cohort—which is extremely unlikely.”
What does it mean?
It means that the mortality rates between recipients of the two vaccines is almost certainly due to the choice of vaccine and not another unseen difference between the two groups of people.
But is this a difference between Moderna’s ability to prevent death or Pfizer’s ability to cause it?
An exchange with a Covid vaccine enthusiast doc…
If you are like Dr. Jonathan Laxton, an Assistant Professor from the University of Manitoba Rady College of Medicine who MedpageToday regards as an “expert” in debunking vaccine misinformation, you would concede that unless we have an idea of how the unvaccinated fared, we cannot know if the folks in this study did better, in general, than those who didn’t get vaccinated. That is what we would expect from an academic physician, and Fellow of The Royal College of Physicians of Canada (FRCPC) who educates the public on misinformation. That is where simple logic leads as well.
But Laxton goes a bit too far. That is what caught my eye when I first took notice of Levi’s announcement of his findings on X and saw this response from Dr. Laxton:
Dr. Laxton believes the study is “garbage” and challenged lead author Retsef Levi to explain to him how his study “raise(s) concerns regarding the potential adverse impact of COVID mRNA vaccination on all-cause mortality” given the fact that there is no unvaccinated control.
Laxton is not a major voice on this or any other topic, but he is a medical doctor and has taken it upon himself to educate “antivaxxers” repeatedly on social media. I am sincerely interested in how these kinds of folks think about things. Maybe he could see his blindspots with a little help from yours truly. Or maybe he could teach me something.
Plainly stated, Laxton assures us there is nothing to see here because the study didn’t have a control group which didn’t receive either vaccine.
Ironically, that is the same reason why “antivaxxers” argue that vaccine trials without saline placebos cannot assess potential harm—and they are right. One cannot prove safety without a true placebo. Similarly, once cannot prove harm exists without one either, but that is not what Levi et al are saying. They haven’t proven harm, they are saying that there are potential adverse effects of Covid-19 vaccinations.
Levi’s study looked at mortality rates from Covid, non-Covid, Cardiovascular deaths and deaths from all causes. In this study if you took the Pfizer series you would have had a 37% greater chance of dying in the following year than if you picked Moderna. The cumulative risk of death seems to increase as time goes on. I agreed with the authors. This raises concerns. If there were dangers from the Pfizer shot that manifested over time, isn’t this exactly what we would be seeing?
In response to Dr. Laxton’s dismissal of Levi’s study, I asked him directly:
“Why would there be a significant difference in all these endpoints between recipients of two different mRNA formulations? That doesn’t raise any questions for you about the safety of the Pfizer shot? What would you do if the same thing happened between two different statin meds? Just close your eyes because there was no placebo group? Aren’t you even a little curious? On what grounds can you say that there’s nothing wrong with the Pfizer shot?”
“What it tells us is that there is a measurable and demonstrable risk associated with mRNA shots. Something that is never acknowledged by those who claim they are Safe and Effective. Of course without an unvaccinated cohort one cannot determine if benefits outweigh risks from this data. But the fact that harm is non zero should give you reason to pause before dismissing it out of hand as being completely irrelevant.”
Let’s say we were looking at these graphs but they were of two different meds. You would still say that the difference in all cause mortality is nothing to be concerned about?
Laxton: “It depends what the control group death rate was. If they were both lower - I would not claim one is higher risk than the other. One would be more effective than the other. Good Lord.”
Right up front Dr. Laxton is letting us know how he looks at things. If the death rate in the unvaccinated is greater than those getting the treatment there is no harm. It’s a very simplistic way of looking at things which runs counter to everything we know about medicine. All drugs and interventions have associated harms, even if the overall benefit when looking at large groups of people may be positive. Somehow, when it comes to vaccines, all that goes out the window. Because I don’t see it that way, I have the blindspot (Good Lord).
Here’s how he tries to convince me:
Laxton: “Let's say the orange line was the unvaccinated control. Now what would this evidence say? Can you see why this study tells us nothing useful without the control?”

Laxton drew hypothetical mortality rates for the unvaccinated in yellow which exceed those of the Pfizer and Moderna recipients. The vaccinated cohorts did better, so what is the problem?
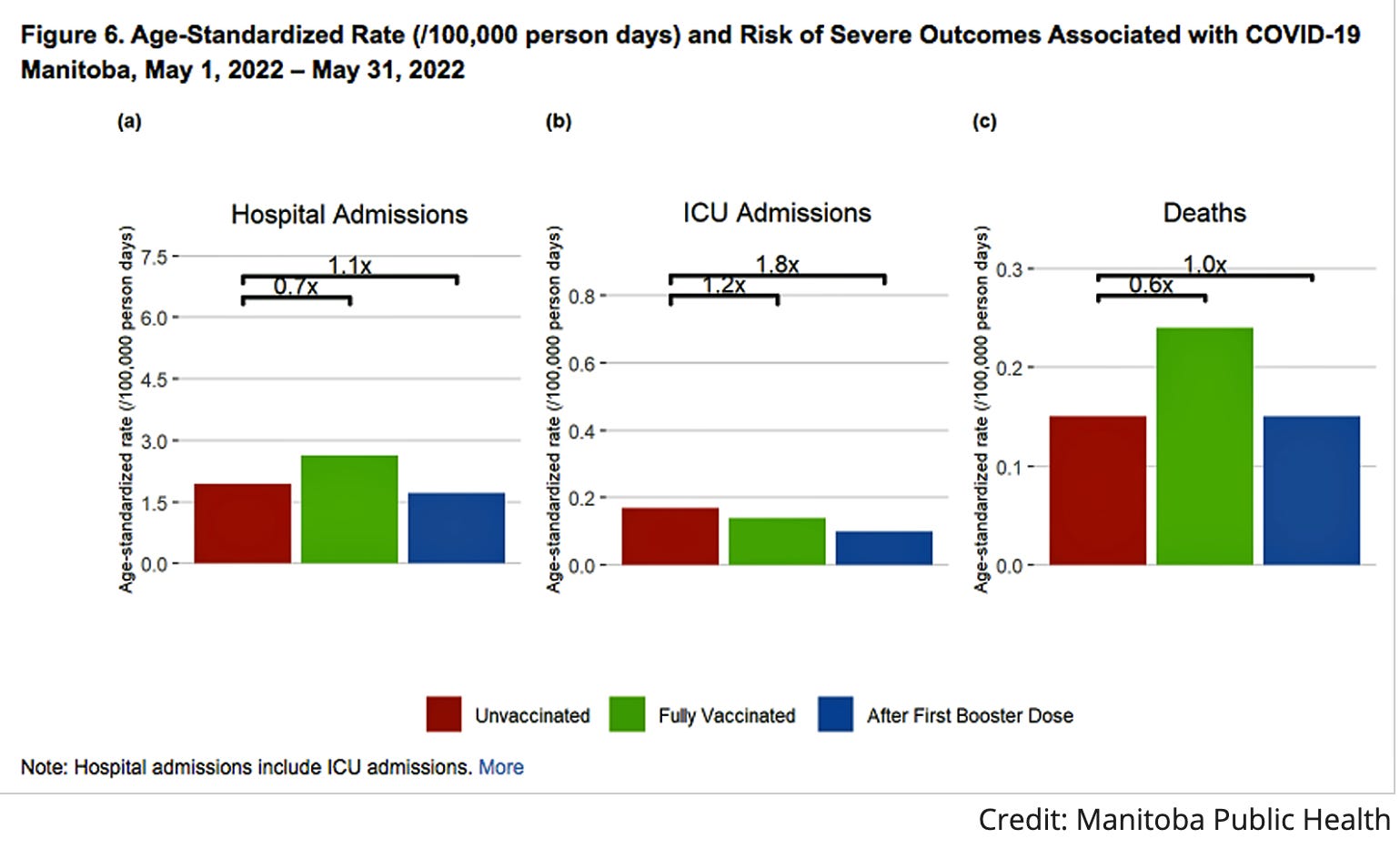
First, this study didn’t look at the unvaccinated, so based on this study alone, there’s no way to know that they did worse in Florida during the period of observation. Interestingly, Laxton’s own province of Manitoba was reporting (Figure 6c) higher Covid-19 Mortality rates in the fully vaccinated compared to the unvaccinated three years ago (around the same time as the observational period of Levi’s study) and then ceased reporting on this metric:
Second, even if unvaccinated mortality rates exceeded those of the vaccinated, how can anyone know if the Pfizer shot was not associated with increased risk of death from specific causes like cancers, strokes, pulmonary emboli, organ failure, myo/pericarditis, etc. compared to Moderna? “All Causes” mean all causes. There’s no way to rule this out. The fact that one vaccine has a substantially greater associated risk of death than the other is extremely suspicious unless you have a preconceived idea that both products are 100% safe. Indeed, that is what Laxton implied earlier.
Referring to his own plot which has mortality rates of the unvaccinated greater than both vaccinated cohorts Laxton says:
Laxton: “This figure does not clearly show harm. In this scenario - it shows Moderna is more effective against death from COVID than Pfizer. Your reply suggests a fixed belief, which is sad.”
Laxton reveals a lot in a few words. He has first assumed that the unvaccinated is at greater risk of dying from all causes but only addresses Covid deaths. Because I am insisting that a safety signal might be nevertheless present, I am the one with the “fixed belief”. He finds this “sad”. Classic gaslighting.
I next pointed out the obvious. Even if Moderna is more effective than Pfizer at preventing Covid-19 deaths, why are deaths from all causes also different?
Me: “Why is ACM higher with Pfizer? Furthermore non Covid deaths were higher with Pfizer. How do you interpret that?”
Laxton: “Because there could have been more COVID during the period driving ACM. Like seriously, this is pretty basic stuff.”
When I exchange with someone on social media I know very well that there is little chance of changing their mind. Nobody likes to admit they have been wrong publicly. I just want to see how they think about things or, in this case, how far they will go to convince me and themselves they are right. Laxton tells us a lot about how his mind works.
It’s pretty basic stuff according to him. It’s so simple that there’s no need to pause and think things through before going any further. More gaslighting.
It still amazes me how the orthodoxy regards those of us who challenge them. Retsef Levi is an MIT scientist. Joe Ladapo is a highly published physician scientist and public figure. Does Laxton really think that they and their colleagues would go to the effort of combing through hundreds of thousands of public health records and begin publishing their analyses because they can’t understand basic stuff? Apparently so.
Moreover Laxton believes he knows why all cause mortality, which includes non Covid and Covid deaths, is higher among those jabbed with Pfizer. “There could have been more COVID during the period…”
In other words, because Pfizer was not as good as Moderna in protecting from Covid deaths, ACM was higher. Yes, that does contribute to ACM.
However the graphs clearly show that the increased risk of Covid deaths incurred with the Pfizer shot is an order of magnitude less than the risk of deaths from all causes. Covid is not driving ACM; it’s deaths from everything else.
Me: “Non Covid deaths were higher. Cardiovascular deaths were higher. At what point will it enter your mind that there’s a risk staring you in the face. Yes. It is basic stuff.”
Laxton: “Right- especially because they didnt match for comorbidities.

Did you even read the study? Also, COVID can drive cardiac deaths as well. Are you unfamiliar with that literature?”
Laxton redirects. He now uses the argument that the two groups were not matched by comorbidities. This is true, however there is very little chance that this would have made any significant impact on the results. Both groups were very well matched on a multitude of potential confounders. Both had an equal propensity to vaccinate (eliminating the healthy user bias). The Rosenbaum framework proves that there would have to be a very significant unaccounted factor between the two groups to explain the difference between outcomes.
Yet I am the one who didn’t read the study.
Laxton also throws in another big assumption: because Covid-19 infection is associated with cardiac deaths, it’s the reason why cardiovascular mortality is different between Pfizer and Moderna. In his mind everything must be due to differences in effectiveness between the two injections. Because I am not attributing every single death from cardiovascular causes to Covid-19, I am the one who is unfamiliar with the literature.
I made one last attempt…
Me: “I agree that that [a difference in comorbidities]would be a confounder as the authors acknowledged. That is not my point. I am challenging your position that this study is "garbage" because there is no unvaccinated control group. I really cannot believe that an academic physician like yourself would look at this data and dismiss it as useless. This should come as a shock if the difference in mortality rates are valid and this significant.
Let's look at your "orange lines" which show a hypothetical mortality plot of the unvaccinated which exceeds the Pfizer and Moderna trajectories. You absolutely cannot conclude that the difference in lives "saved" is soley due to a difference in effectiveness between the shots. Efficacy in the trials and Effectiveness in the post marketing data is defined by Covid-19 mortality only. By your logic, anyone who dies of a heart attack must have succumbed to the event because of Covid-19. That's ridiculous prima facie.
What does a Non-Covid death mean to you exactly? A fatality from a rupture of varices? Liver failure? Aortic dissection? Subarachnoid hemorrhage? All of these were from Covid because they have been reported in the literature? Myocarditis? PEs? CVAs? You do realize that these are also associated with mRNA vaccines too, right? But according to you we can just chalk them all up to Covid-19 and not any difference in the risk between Pfizer and Moderna? Please explain how you can come to that conclusion.”
In this final exchange I am pointing out the absurdity of his position. If he believes that the stunning difference in mortality can only be due to the difference in each vaccine’s ability to prevent Covid and Covid related deaths, then every single one of the deaths among the 1.4 million people in the study were directly or indirectly due to Covid and nothing else.
His response:
Laxton: “PEs and CVAs are NOT associated with mRNA vaccines. I've already explained my conclusion. You are now just sea-lioning.”
PEs: Pulmonary Emboli (blood clots entering the pulmonary circulation)
CVAs: Cerebrovascular Accidents (Strokes)
Sea-lioning: “A subtle form of trolling involving "bad-faith" questions. You disingenuously frame your conversation as a sincere request to be enlightened, placing the burden of educating you entirely on the other party. If your bait is successful, the other party may engage, painstakingly laying out their logic and evidence in the false hope of helping someone learn. In fact you are attempting to harass or waste the time of the other party, and have no intention of truly entertaining their point of view. Instead, you react to each piece of information by misinterpreting it or requesting further clarification, ad nauseum.”
Conclusion
This is the kind of exchange that frightens me to the core. How much of the medical establishment thinks like this doctor? Laxton uses various methods to solidify his position when challenged. Reframing, redirecting, over simplification. Is there a way through this kind of cognitive blockade? It is important to me because unless we understand what we are up against righting the ship may be impossible.
Please leave your comments.
There is an elephant in the room. WHY ISN'T THERE AN UNVACCINATED CONTROL GROUP?
In my experience, it could be because the study becomes unpublishable if it clearly demonstrates vaccine harms. (Not literally unpublishable, but none of the mainstream journals will consider it. I have tried. Others tell me of the same experience.)
As Surgeon General, Dr Ladapo presumably has access to the necessary Florida health data to extend the study with an unvaccinated control group. He chose not to. Maybe it's because he has an irrational prejudice against vaccines, and he doesn't want to show the world how many lives the mRNA shots have saved. That's Laxton's presumption. Or maybe politics has made vaccine safety a very touchy issue, and Ladapo is being strategic about bringing out the safety data gradually, and with impeccable statistical foundation.
why they must deny..(according to Charles Eisenstein)
"Why must they be wrong?(antivaxxers) Because if they are right then the whole edifice of modern society — its systems of knowledge production, its public institutions, academia, government, and the ideology of progress — must be unsound, for the core medical practice of vaccination is embedded within them. You can’t believe “We got this one item wrong” without impugning the rest of the edifice along with it."