


Did the mRNA shots really save millions of lives?
Yesterday Dr. Meryl Nass and I chatted about my return to clinical medicine, the scary stuff the W.H.O. is planning and the biggest misconception about the mRNA "Vaccines"


I had the opportunity to speak with friend (and inspiration), Meryl Nass, on “Good Morning CHD” yesterday.
Like me, Meryl is a fellow MIT grad and practitioner of Vipassana. She also happens to be a world authority on Anthrax, the Anthrax vaccine and bioterrorism. She has given Congressional testimony a half dozen times.
After 41 years with an impeccable record as a primary care physician in MA and Maine, her license to practice medicine was suspended for frivolous reasons in the end. However she was brought to the ME Board of Medicine's attention for treating Covid with Hydroxychloroquine, a fully licensed drug with remarkable antiviral properties and a safe and potent treatment for a wide range of ailments from Malaria to Rheumatoid Arthritis.
Any physician in the US with a medical license can use a licensed drug for anything they want to. It's called off-label use. I could use HCQ to treat depression if I wished. However, if a doctor used it to treat Covid, it would end their medical career. Every doctor in this country should be outraged at this overreach.
In our conversation I recounted my return to clinical anesthesiology in a busy community hospital and the kind of conversations I have been having. I am encouraged. Health care professionals, especially nurses and mid-level providers have been very open to the possibility that there is a coherent counter narrative to the “safe and effective” mantra.
Here’s a link to the show.
About a year ago, I had the chance to invite a group of three nurses to examine the VAERS (Vaccine Adverse Event Reporting System) website after they reluctantly admitted that they had some concerns about the Covid “vaccine’s” safety. They couldn’t believe that the CDC was officially collecting reports of vaccine injury. I wish you could have seen them crowd around the computer reading adverse event reports, one after the other, confirming their suspicions about what they had seen during the first two years of the vaccine roll-out.
I have also had conversations with some whose family members are convinced that they were suffering long-term, devastating vax side-effects, or others who are trying to make sense of why one or more of their young and healthy friends suddenly suffered from devastating diseases like myocardial infarctions and aortic dissections.
Another colleague was recounting her shock and dismay at what happened when a physician, in a desperate attempt to treat a dying patient, tried to order Ivermectin, an exceedingly safe, licensed medicine with good efficacy against Covid especially if given early. The doctor’s order placed in the hospital’s computer system triggered an immediate alert to the Pharmacy and senior medical staff who put a stop to it. Meetings were held. Only after several discussions where it was made clear that the patient’s family were demanding its use was the medicine given.
“In all my years, I have never seen such a response from so high up with regard to a pharmaceutical intervention.”
It seems that there is at least a large minority of providers at my facility who believe that something fishy has been going on.
Yet despite suffering multiple bouts of Covid after multiple jabs, medical professionals at my facility are still unwilling to challenge the idea that the mRNA shots have saved millions and millions of lives. It is this belief which allows them to swallow the reality that yes, some have been injured, but in the end they did more good than harm.
But did they really? Our only view into this question comes through official data sets that are tallied, compiled and distributed by three letter agencies like the CDC and the ONS (Office of National Statistics). You can trust them if you like, but why should you?
The mRNA shots never worked
Over two years ago, Professor Emeritus Norman Fenton (Queen Mary University, London) and colleagues proved that the official statistics coming from the ONS misclassified people’s vaccination status in their All Cause Mortality (ACM) data. This directly led to the exaggeration of mortality rates in the unvaccinated population, potentially hiding vaccine related mortality.
The same faulty methodology is openly being used in their assessment of Vaccine Effectiveness. Here the ONS states how they are classifying people by vaccination status:
unvaccinated: those with no vaccination or who were vaccinated with a first dose less than 21 days ago
second dose: those who were vaccinated with a second dose at least 21 days ago to earliest of less than 91 days after second dose or less than 21 days after third dose
What is so important about these definitions? First, if anything happens to someone within three weeks of getting their first shot (infection/hospitalization/death) it gets lumped into the unvaccinated pile. This will artificially increase the incidence of that outcome among the unvaccinated.
Second, if anything happens to someone within 21 days after a second dose, that outcome is excluded from the “second dose” category. This will artificially decrease the incidence of that outcome among those considered having completed the primary series.
Vaccine Effectiveness being directly related to the ratio of the incidence of an outcome in the vaccinated group compared to the unvaccinated group—viola! You have created vaccine effectiveness where none existed!
Is this really such a big deal? Fenton aptly explains this here by taking a hypothetical vaccine with no effectiveness and shows how big an effect this might have:

It turns out that the Effectiveness of a placebo can look a lot like the Vaccine Effectiveness of an mRNA shot depending on how quickly the public gets vaccinated.
So that’s what the ONS is doing. What about our CDC? It turns out that the CDC is not as audacious, but they are doing something deceptive too. Though not overtly taking outcomes from the vaccinated and including them with the unvaccinated, they are, it seems, excluding outcomes in those vaccinated within two weeks of completing their primary series, but including them in the the vaccinated population.
In other words, if you just got the second shot and get Covid, it doesn’t count against the vaccine but you get counted as another person who is vaccinated. How do we know this is what they are doing?
Briefly, the CDC categorizes people into three categories: unvaccinated, vaccinated and partially vaccinated. The latter being those who have received at least one jab and are not quite outside a 14 day window from receiving their second one. The deception is how they define incidence rates:

The above is a screenshot from the CDC website year ago. The key point is that,
“Weekly age-specific incidence rates by vaccination status were calculated as the number of cases or deaths divided by the number of people vaccinated with a primary series, overall …”
What do they mean by the number of people vaccinated with a primary series, overall?
Are they including those who were vaccinated within 14 days or not? When it comes to outcomes, they explicitly excluded those which occur in those who are recently vaccinated, so they should be excluding them from “the number of people vaccinated with a primary series”. If they included them, they are spreading outcomes over an artificially larger population. This will automatically exaggerate the vaccine’s effectiveness.
But the number of people in this limbo category, the partially vaccinated, is for most of the pandemic, tiny compared to those the CDC considers to vaccinated and unvaccinated. Could excluding outcomes in this group while including them in the vaccinated group really distort things appreciably?
As I will demonstrate, it would be a very big deal. I wrote to the CDC asking for clarification. Some days later I got a response. The person on the other end asked me to cite the page from their own website which pertained to my question. I went back and their definition of Incidence Rate Estimates disappeared.
In this essay, I use Dr. Fenton’s approach by showing how much “fake” effectiveness gets generated by using this faulty approach:

As explained above, the key determining factor of fake effectiveness is the rate of vaccine uptake by the population. Using stats from Our World in Data I estimated that the effectiveness of a placebo using what I believe is CDC’s methodology would have looked like this:
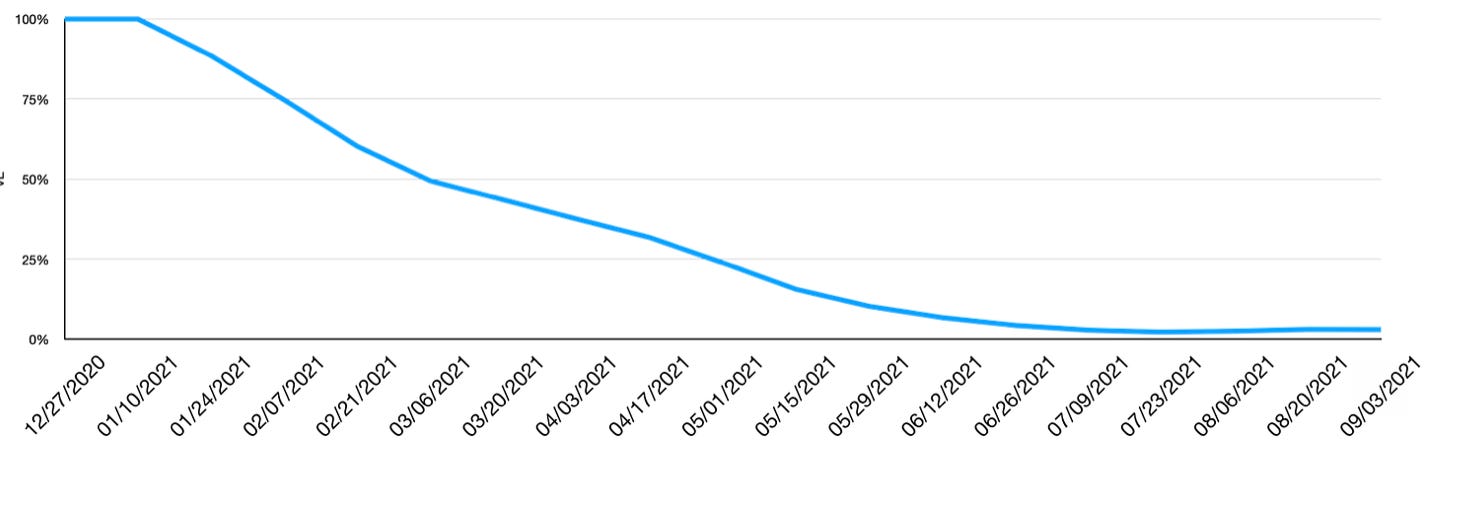
That graph should look familiar. But it’s not the effectiveness of the mRNA vaccines over time, it’s of a hypothetical shot with no efficacy.
At the beginning of 2021: 100% effective! Go get your primary series! (You’ll also be treated with Target gift cards and Krispy-Kreme donuts for your compliance)
But by August…The primary series isn’t working anymore. Go get your booster!

But if the observational data demonstrated that the vaccine did no better than a placebo, why did the trials show that they were 95% effective??
There could be several reasons for this. This article which recently appeared on The Defender summarizes several papers which identify biases in the trials and estimate how they exaggerated efficacy. Excluding cases amongst the recently vaccinated trial participants, aka “case-counting-window” bias, was in play during the vaccine trials too.
In my discussions with colleagues who are beginning to open their eyes to what has really transpired over the last four years, this issue is vitally important. If we cannot acknowledge that these products may very well have done next to nothing good there is little chance we will be prepared for what is in store for us…
The Pandemic Treaty and International Health Regulations
Dr. Nass finished the conversation by summarizing what is being codified, largely outside of the public’s attention. The Pandemic Treaty and amendments to the IHR would, among other things:
Allow for the development of labs in participating nations to do gain of function research under the guise of pandemic preparedness
All products of this dangerous research would be shared with the W.H.O. and participating nations
Vaccines, using the flawed mRNA platform, would be developed at hyperspeed, a 100 day time frame with severely curtailed testing periods
There isn’t any plan for compensating those who might be injured from said vaccines
The W.H.O. gets to decide what constitutes mis and dis information around these matters
More details and informational material can be found at Dr. Nass’s organization, Door To Freedom.
Peter Doshi raised the right questions about two categories: "suspected Covid" and "protocol violation".
https://blogs.bmj.com/bmj/2021/01/04/peter-doshi-pfizer-and-modernas-95-effective-vaccines-we-need-more-details-and-the-raw-data/
Great discussion between you and Dr. Nass. I hope the video gets some reach outside of the CHD website.